Curi Bio’s ribbon cutting in April 2025 for its new headquarters on Seattle’s waterfront. Elliot Fisher, co-founder and chief business officer, cuts the ribbon with a sword while CEO Nicholas Geisse holds a pair of scissors. (Curi Bio Photo)
Seattle biotech startup Curi Bio, which enables the screening of new drugs using cells and 3D tissue models derived from human cells, announced $10 million in new funding.
Curi Bio’s customers include large biopharmaceutical and biotech companies such Novo Nordisk, Eli Lilly, Astrazeneca, Pfizer, Boehringer Ingelheim, UCB, Novartis and others. Its Series B round was led by Seoul-based DreamCIS, which supports biopharma R&D through extensive research services.
“We are thrilled to partner with DreamCIS, who shares our conviction that drug discovery urgently needs more human-relevant data at the preclinical stage,” said Michael Cho, Curi Bio’s chief strategy officer, in a statement. “The vast majority of new drugs fail in human clinical trials because preclinical animal and 2D cell models have failed to be good predictors of human outcomes.”
Curi Bio’s platform integrates bioengineered tissues created from induced pluripotent stem cells (iPSCs) with data collection and analysis. The additional funding will expedite its development of new platforms for cardiac, skeletal muscle, metabolic, smooth muscle and neuromuscular diseases, the company said.
The Seattle area is a hub of life science and biotech companies, including numerous efforts focused on AI-assisted research. Researchers have emphasized the need to test computer-generated drug candidates in the lab to verify their capabilities and impacts.
“Curi Bio’s unique integration of cells, systems, and data is a paradigm shift for preclinical drug discovery,” said Jeounghee Yoo, CEO of DreamCIS. “We were incredibly impressed by the company’s innovative platforms and their ability to generate functional data from 3D human tissues at scale.”
Curi Bio has raised $20 million from investors and $12 million from federal grants.
The company spun out of the University of Washington a decade ago as NanoSurface Biomedical. In April, Curi Bio celebrated the opening of its new 13,942-square-foot headquarters and research facility on the Seattle waterfront.
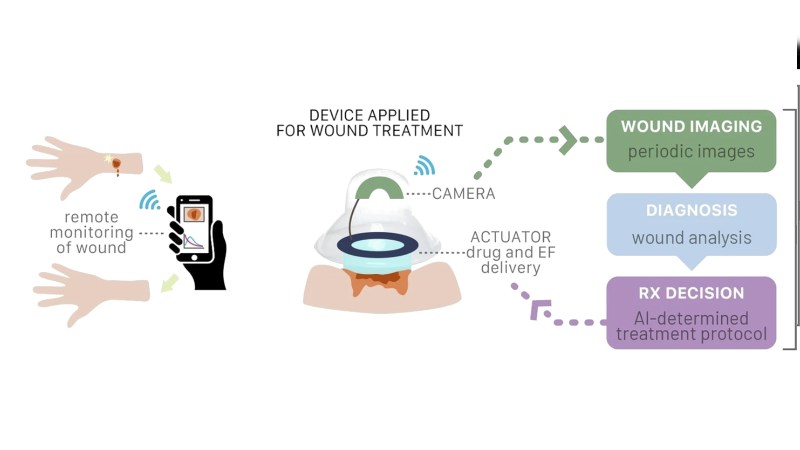
If you get a small cut, you might throw a plastic bandage on it to help it heal faster. However, there are fancier options on the horizon, like this advanced AI-powered smart bandage.
Researchers at UC Santa Cruz have developed a proof-of-concept device called a-Heal, intended for use inside existing commercial bandages for colostomy use. The device is fitted with a small camera, which images the wound site every two hours. The images are then uploaded via a wireless connection, and processed with a machine learning model that has been trained to make suggestions on how to better stimulate the healing process based on the image input. The device can then follow these recommendations, either using electrical stimulation to reduce inflammation in the wound, or supplying fluoxetine to stimulate the growth of healthy tissue. In testing, the device was able to improve the rate of skin coverage over an existing wound compared to a control.
The long-term goal is to apply the technology in a broader sense to help better treat things like chronic or infected wounds that may have difficulty healing. It’s still at an early stage for now, but it could one day be routine for medical treatment to involve the use of small smart devices to gain a better rolling insight on the treatment of wounds. It’s not the first time we’ve explored innovative methods of wound care; we’ve previously looked at how treatments from the past could better inform how we treat in future.
Imagine waking up one morning, scrolling through your portfolio, and realizing the stock you almost sold last quarter has just jumped 36% overnight. That’s not a dream-it’s Globus Medical (GMED) after its blowout Q3 results. If you’ve ever wondered how innovation, precision, and timing collide in the medical tech world, this stock is your masterclass. Between robotic surgeons, record-breaking buybacks, and near-zero debt, GMED isn’t just fixing spines-it might fix your portfolio’s posture too.
Operations: Precision Engineering Meets Global Reach
Globus Medical designs and sells life-changing devices for spine, trauma, and joint reconstruction, powering over 10 million procedures worldwide. Their crown jewel? The ExcelsiusGPS robot, now in 500+ U.S. hospitals, slashing surgery times by 30% and errors to near-zero.
With 5,300 employees across 64 countries, revenue tilts 60% U.S.-heavy but expands via smart acquisitions like Nevro’s pain-tech, tapping a $3 billion neuromodulation market. It’s not just hardware-software like Surgimap plans surgeries virtually, turning complex ops into seamless wins.
Financial Firepower: Cash Machine in Overdrive
Q3 2025 was a rout: revenue hit $769 million (up 23% YoY), smashing estimates by $34 million, with non-GAAP EPS at $1.18 (up 43%). Free cash flow? A record $214 million, fueling $256 million in YTD buybacks.
Globus Medical Stock Surge: From Underdog to Momentum Monster
Analysts swarm:
BofA’s „Buy” at $91 cites 16% EPS CAGR through 2027;
Truist’s $93 targets 11x EBITDA.
Volatility? Sure, but with 50% two-year revenue CAGR, it’s the kind that rewards holders.
The stock price has risen by more than 527.04% since the IPO.
Returns to You: Buybacks Over Boring Dividends
No dividends here-Globus prioritizes reinvestment in R&D (12% of sales) and growth. Instead, a $500 million buyback bonanza signals rock-solid confidence, erasing 2% of shares YTD at bargain prices. It’s smart capital allocation: why pay out when you can compound at 30% margins? For yield chasers, it’s zero-but for total return hunters, those repurchases juice EPS by 5–7% annually.
Rivals in the Ring: Globus Packs a Punch
In the $13 billion spine arena (growing 6% CAGR), Globus ties Medtronic at 25% share, nipping at heels with robotics edge over J&J’s (10%) procedural focus and Stryker’s (12%) breadth. Acquisitions like NuVasive doubled scale without the integration headaches of past deals. IP moat? Ironclad-$9.5 million patent win vs. Life Spine deters copycats. While peers chase diversification, Globus lasers on spine, outpacing with 38% five-year revenue CAGR vs. Medtronic’s 5%.
Data as of Nov 10 close; yields reflect trailing 12 months. GMED’s zero yield underscores growth reinvestment, trading at a peer discount on P/E.
Headlines That Hit Hard: Earnings Ignite a Rally
November 6’s Q3 bombshell- 23% sales leap, EPS crush, Nevro turning profitable now-catapulted shares 36%, adding $4 billion in market cap overnight. Why the jolt? It crushes fears of acquisition indigestion, proving Globus can integrate and accelerate (U.S. spine up 10%). Downside? R obotics dipped 27% on hospital budget squeezes, but it’s just 4% of sales. Net impact: a 20% EPS guide hike signals $4+ earnings by 2027, potentially $100+ stock. For investors, it’s validation-buy the dip, ride the wave.
X-Factor: What Wall Street Whispers
Investment Insights
Globus Medical’s profitability has been under pressure in recent years. The company’s Net profit margin has declined to 4.09%, continuing a multi-year downtrend. Gross margin has also narrowed slightly, now standing at 59%, still near its long-term average but showing signs of cost inflation and operational strain.
A closer look reveals that General and administrative expenses are weighing heavily on performance, absorbing 66% of Gross profit. This high expense ratio signals that management is investing heavily in scaling operations and infrastructure — a hallmark of an aggressive growth phase.
Rapid Expansion Driving Operational Costs
Globus Medical is clearly in the midst of a strong expansion cycle. Over the past five years, the company’s headcount surged by 165% to more than 5,300 employees, reflecting rapid integration following acquisitions and continued investment in R&D and global distribution.
Such growth inevitably brings short-term pressure on profitability ratios, but it positions the company for higher long-term revenue potential and operating leverage once integration costs normalize.
Strengthened Balance Sheet Through Full Debt Repayment
This strategic deleveraging move reinforces investor confidence, particularly in an environment where interest rate volatility and capital efficiency are in focus.
Investment Outlook: A Growth Stock with Moderate Risk
Following its improved capital structure, Globus Medical’s Investment Scoreboard rating stands at 69, classifying it as a solid investment-grade growth stock. We expect the company’s share price performance to outpace its long-term historical CAGR of 12.35%, supported by expanding markets and product innovation.
Investment attractiveness
Globus Medical Stock Forecast
2025–2029 Price Targets:
Trading and investing tips
At the time of writing, the stock price has surged sharply following strong positive news, yet it still remains well below its previous all-time high (ATH). This presents a favorable opportunity to open a new position or add to an existing one, as under the current supportive market conditions, a meaningful correction appears unlikely.
Despite the roughly 40% price increase, the stock is still reasonably and fairly valued compared to fixed-income instruments. Even at current levels, the expected annual return in an optimistic scenario could reach up to 19% on average per year.
Conclusion
Globus Medical’s story is one of surgical precision-literally and financially. It’s rare to find a company that cuts operation times and boosts operating margins. With robots doing the heavy lifting and management trimming the debt fat, GMED looks fit for long-term growth. And let’s be honest-if your back ever needs a fix, wouldn’t you rather it be done by a company that just gained 36% in a day?
Have you already invested in this company’s stock? Leave a comment-we’re closely following this stock!
Share the article with friends and colleagues!
Donate for this awesome analysis:
Originally published at https://aipt.lt on November 13, 2025.
Cannabis has a bad reputation when it comes to building up a tolerance. Countless articles describe the problem: you start using cannabis and it works great, but after a few weeks you find you need more. You increase your dose, only to soon find that this new dose is also insufficient — it just doesn’t get you ‘high’ the same way.
The prescription for this problem is usually to go on a tolerance break, a few weeks where you stop using cannabis and let your system reset. When you go back to using cannabis again, your tolerance will be back down to where you started. The message being communicated is clear: tolerance isn’t something you want to have.
But developing a cannabis tolerance isn’t all bad. For many, especially medical patients, it is a crucial factor in their cannabis use. Many medical patients starting cannabis worry about side effects like difficulty thinking, problems with memory or lack of coordination.
One of the great benefits of developing a tolerance to cannabis is that many of these side effects go away: Studies show chronic cannabis users do not suffer from the same disorienting effects that leave occasional users unable to do everyday tasks, such as driving).
I saw this firsthand as a cannabis patient. For me, cannabis was always disorienting. It wasn’t a bad thing, but it did make it impossible to get much done while under the influence.
I remember marvelling at a close friend and classmate who could smoke throughout the day while remaining completely normal. He would go to class, have complex conversations about analytic philosophy, work on his doctorate — all while using cannabis.
When I asked him about it he explained that he had a high tolerance. He was just used it.
At that time, I was dealing with intense chronic pain and missing a lot of school and work due to these struggles. Cannabis helped, but I was only using it at night when I didn’t have any work to do. It was like a time-out from the pain, but it didn’t help me with the real problem — my inability to work when I was in pain.
My friend suggested something that ran counter to everything I had read — I should build up my tolerance.
“Smoke right before you write that paper” he suggested. “It will be weird for a few days, but then you’ll be used to it”.
Time to Build Up a Cannabis Tolerance
To my surprise, he was right. Within a week of starting to use cannabis during my regular work and school activities, I was no longer feeling the disorienting side effects. I was free. While I still had relief from my pain and anxiety, I was thinking clearly and felt… normal.
While I worried my cannabis tolerance building would lead to continual increases in use, at a certain point my tolerance increases seemed to plateau: I have been on a relatively stable dose for the last five years. If I use the same strain of cannabis for too long, I develop a tolerance to that strain and need to switch it up to keep getting relief. Otherwise, I haven’t experienced any tolerance-related problems and always avoid taking tolerance breaks now.
While tolerance breaks are fantastic for recreational users or those with occasional medical needs, I never suggest them for medical patients who have chronic issues they are managing. Just like you would be unlikely to have a doctor suggest you take a few weeks off from an antidepressant or a heart medication if you are using cannabis for daily medical needs, interrupting this can be disruptive and confusing for your body. And of course, any symptoms you were managing will no longer be getting the help they need.
Still, last summer, I was forced to take a tolerance break: I got a lung infection (unrelated to the cannabis) which was aggravated by smoke, so I spent months unable to use my medicine.
When I started to smoke again a few months later, my cannabis tolerance was back at its starting point and I experienced tolerance free cannabis use again. I was totally useless! So, I spent the next few weeks building my tolerance back up. Only then was I able to again use cannabis effectively as medicine.
I thought I might be able to use a lower dose after such a long break, but I quickly found myself back at that stable dose I had been using for years. For all the discomfort of the break, it turned out that I did best on the dose I had already been on.
While tolerance breaks are great for some (and there are certainly medical and recreational users alike who swear by them), for others developing and keeping a certain level of tolerance may be the better route. This can vary drastically from person to person based on their needs and biochemistry.
As a patient consultant, I often work with clients to track their cannabis experiences in a journal. Looking back over a few weeks of entries, many of them are able to better understand what is working for them and what isn’t.
TELL US, has tolerance affected your cannabis experience?
Our bodies all have a network of cannabinoid receptors that is vital to the health of all mammals: the endocannabinoid system. The ECS is a vast network of chemical compounds and receptors (namely CB1 and CB2) that regulate our most basic functions – sleep, appetite, mood, the immune system, inflammatory response, aging and memory. Endocannabinoids even produce feelings of relaxation and euphoria similar to those which come from ingesting cannabis.
Aside from regulating essential everyday functions, the ECS maintains the body’s homeostasis down to the cell level by reversing damage in whatever way necessary. In cancer patients, for instance, cancer cells can be programmed to kill themselves when endocannabinoid levels increase.
But as with most things, balance within this system is key. An overly inhibited CB1 receptor may lead to moodiness, depression and a suppressed immune system. On the other hand, an over-activated CB1 can increase risk of psychoactivity, inflammation, diabetes, obesity and cardiovascular problems. One study found that a highly sensitive endocannabinoid system is linked to almost all chronic diseases. So, a balanced ECS is fundamental to good health.
Consuming cannabis is one fun and easy way to optimize the ECS. But not everyone has the freedom to enjoy this medicinal plant. Here are our top five simple ways to boost the endocannabinoid system without the aid of marijuana.
Drink Less Alcohol
Martin Lee, director of Project CBD and author of “Smoke Signals: A Social History of Marijuana – Medical, Recreational and Scientific,” explained the problem with drinking:
“Alcohol is a poison that causes an acute stress response upon occasional consumption, which, in turn, provokes a temporary uptick of endocannabinoid activity as a protective response against stress,” Lee said. He added that while occasional drinking probably wouldn’t harm the ECS, “chronic alcoholism has the opposite effect, resulting in a depletion of endocannabinoid tone due to the wear and tear of too much stress. A low endocannabinoid baseline level makes a person more vulnerable to disease.”
Get Bodywork Treatments
A study by Auckland’s Unitec Institute of Technology showed that levels of anandamide — a cannabinoid responsible for feelings of bliss and joy — more than doubled after patients received osteopathic manipulative medicine treatments. This therapy can take various forms, including chiropractic, physical therapy and massage. Even acupuncture has a positive effect on the endocannabinoid system, so there’s never been a better excuse to take a spa day.
Eat Leafy Greens
If smoking frosty greens is not an option, then eating leafy greens will suffice. Along with oregano and black pepper, leafy greens contain beta-caryophyllene, a terpene that activates the CB2 receptor and is believed to have high potential for combatting inflammatory conditions and autoimmune disorders.
Eat More Omega-3s
Omega-3 fatty acids are essential for a well functioning ECS. Some scientists say that without them, CB1 receptors may not form correctly, which could lead to “impaired emotional behavior.” While fish oils are widely considered one of the best sources of omega-3s, hemp is an excellent alternative. Whether in seed, oil or protein form, hemp’s omega-3s can help keep your ECS functioning properly.
Exercise
German researchers have shown that “runner’s high” is not actually caused by an endorphin rush, but instead is a result of an increase in endocannabinoid production. And running isn’t the only activity that produces this effect. Any exercise can lead to an increase in endocannabinoids, so long as the activity doesn’t feel forced. The body interprets forced exercise as a stressor, which can actually produce the opposite effect and decrease endocannabinoid receptor signaling. So, dust off the yoga mat, jump up and down on a trampoline or even go out dancing to maintain a healthy endocannabinoid system.
Originally published in the print edition of Cannabis Now.LEARN MORE
TELL US, how do you combine cannabis with other wellness techniques?
Cannabis topicals are having a moment. From
A-list celebrities using Lord Jones balms to soothe aching feet at the Golden
Globes to professional athletes debuting their own line of muscle rub,
transdermal products infused with cannabinoids seem to be everywhere.
But it isn’t just millennials and the Hollywood elite jumping on the bandwagon. An increasing number of senior citizens are also turning to topicals, often desperate to alleviate a painful and often debilitating condition that affects nearly 54 million American adults: arthritis.
The disease, which causes aches, swelling and stiffness in the joints and muscles, is typically treated with a combination of medications including steroids and opiates, which may have dramatic side effects. However, cannabis is becoming a popular and viable alternative. Infused creams and lotions work when the products’ cannabinoids bind to the network of cannabinoid receptors called CB2 receptors on the skin, without needing to enter the bloodstream. This means people using topicals infused with psychoactive cannabinoids such as THC will not feel a cerebral effect — only localized relief. Transdermal patches, however, do allow the cannabinoids to enter the bloodstream and travel to receptors in the brain, but because the release is so slow, it’s also unlikely to impart a high feeling.
While research on the efficacy of topicals is limited, there have been some promising results. A 2015 study published in the European Journal of Pain found that, when applied transdermally to rats with arthritic joints, the cannabinoid CBD (cannabidiol) offered relief. Another study conducted in 2017 on rats with osteoarthritis (the most common type of arthritis, wherein bone cartilage breaks down over time) concluded CBD prevents pain and nerve damage. In fact, scientists are also exploring evidence that concludes CB2 receptors themselves may be responsible for regulating inflammation — one of the main issues arthritis causes.
The science is still early, but according to Radicle Health founder and nurse Eloise Theisen, CBD topicals appear to help with inflammation and itchiness, but people should try a THC topical — or a combination of THC and CBD — if they’re not finding relief from a CBD-only product.
Since the average senior citizen in the United
States takes around five prescription medications daily, concerns about
interactions between drugs, side effects and potentials for abuse have many
seeking another way.
And since those who might be averse to getting high from smoking or eating cannabis are often not intimidated by using a non-psychoactive cannabis balm, topicals offer a way to discover the healing properties of cannabis while eliminating the fear of Grandma and Grandpa getting too buzzed.
‘Once He Went Off the Pharmaceuticals….’
Karen Rumics Averill is a 63-year-old business
owner from Oregon who began making her own cannabis-infused topicals a few
years ago to help her husband. He was suffering from a severe type of arthritis
called ankylosing spondylitis, also known as “curved back syndrome.”
“He was initially put on Enbrel, which is an
injection, and he was actually receiving twice the dose that is normally
required,” Averill said. “Then, [the doctors] put him on Oxycontin and Vicodin
and then all of a sudden one day, at two in the morning, we’re rushing him to
the emergency room for a bleeding ulcer and they had to remove him from all of
those drugs.”
She believes the drugs her husband had been
prescribed were actually making his condition worse.
“Once he went off of [pharmaceuticals], he became
more mobile, more active. He wasn’t comatose on the couch because he was
over-medicated.”
Averill began experimenting, utilizing byproducts
from top-shelf indica strains to infuse in coconut oil, creating a THC-infused topical.
“Actually, my 94-year-old aunt is now using it
for her arthritis. She called me
yesterday and said it works great!” Averill said.
Bringing Seniors to Cannabis
For many within the cannabis industry, one of the biggest challenges is getting accurate information to the general public — without being overwhelming or unconvincing. After getting phone call after phone call from seniors asking about their transdermal product, the team at NanoSphere Health Sciences decided they needed to focus not on getting their products to seniors, but on bringing the seniors to them.
“A lot of times, the way that a senior gets our
product is because a niece or nephew, granddaughter, son or daughter has gone
in, bought them the product and then told them that they need to use it, versus
them actually going into the dispensary and purchasing the product themselves,”
said Crystal Colwell, marketing director for NanoSphere.
So the company decided to partner with several dispensaries in their home state of Colorado, offering residents of nearby assisted living facilities and 55-plus communities round-trip bus rides to their locations in order to educate them on the many useful applications of cannabis. They also work with the non-profit group Realm of Caring in order to further their outreach towards the senior citizen demographic. Colwell says the feedback has been remarkable.
“We had one woman who had such severe arthritis
in her hands that she was unable to open her hands all the way,” Colwell said.
“One of her most favorite things to do is to write letters and handwritten
notes. She started using NanoSerum on her hands and she was using it once a day
for a month and after the first month she was able to open her hand and hold a
pen or a pencil in her hand again. Within a two-month time span, she was
actually able to write handwritten notes again.”
Colwell adds that while it will take time to
dismantle all the misinformation about marijuana and the ways it can be
consumed, topicals offer a non-threatening introduction to a medicine that
could make all the difference.
“A lot of misconceptions that senior citizens have is that the only time you can get relief from cannabis is if you smoke it or you ingest as an edible,” she said. “Once they learn that there are alternative applications, that’s when they become intrigued and it gets their mind going.”
Originally published in the print edition of Cannabis Now.
Dr. Tod Mikuriya was a critical force in the
successful and ground-breaking effort to legalize medical marijuana in
California in the 1990s. Now his papers
are available to researchers through a newly archived collection at the
National Library of Medicine.
The Berkeley psychiatrist, who died in 2007, was hailed as the grandfather of the medical marijuana movement, backing up the activists with unimpeachable scholarly chops to the rage of the Drug War establishment. It was hard to assail his credibility, as he had actually headed up the National Institute of Health’s cannabis research program in the 1960s before defecting to the side of the people being studied, so to speak.
An ‘Inappropriate Attack of Curiosity’
Mikuriya was born in a rural part of
Pennsylvania’s Bucks County in 1933, to mixed German and Japanese immigrant
stock. This obviously made him the target of prejudice during his childhood in
World War II, an experience to which he would later attribute his rebellious
streak.
Mikuriya received his bachelor’s degree in psychology from Reed College in
Oregon in 1956, before serving a medic in the Army. He then went to medical
school at Philadelphia’s Temple University, where the turning point in his life
occurred.
As he would years later relate to video-journalist Ruby Dunes on the sidelines of a cannabis conference in Santa Barbara, in 1959 Mikuriya was “struck by an inappropriate attack of curiosity” after reading an unassigned chapter in a pharmacology textbook that mentioned the widespread medicinal use of cannabis in the United States before it was outlawed in 1937.
He was sufficiently intrigued that on summer break between semesters that year, he overcame his ingrained fear and traveled to Mexico to seek the stuff out, buying a small quantity from a street-dealer. Nothing would ever be the same for him.
In 1966, Mikuriya began directing the drug addiction treatment center of the New Jersey Neuropsychiatric Institute, at Princeton. That same year, he travelled to Morocco’s hashish heartland of the Rif Mountains, where he smoked kif with Berber tribesman who had resisted French colonial efforts to stamp out cannabis smoking.
It was also during this period that he discovered and immersed himself in the works of Sir William Brooke O’Shaughnessy, the Irish physician who researched the long tradition of medicinal use of cannabis in India in the 19th century. Mikuriya came to view O’Shaugnessy as a “personal hero.”
Mikuriya was also among the first scholars to re-explore the findings of the Indian Hemp Drugs Commission Report, the 1894 study ordered by British colonial authorities to examine the supposed cannabis problem in the subcontinent, which instead determined that use is “either harmless or even beneficial.”
In 1967, Mikuriya became a researcher at the Center for Narcotics & Drug Abuse Studies of the National Institute of Mental Health (NIMH), itself a division of the National Institutes of Health. This agency was the predecessor of today’s National Institute on Drug Abuse (NIDA). There, he headed up what he would later call the government’s “first overground cannabis research program.” (He would learn there was a “concurrent secret study” going on at Edgewood Arsenal in Maryland, linked to the CIA’s search for truth serums and psychotropic warfare agents.)
He was dispatched to California for the study, to observe the habits of the hippies who were then bursting upon the scene. But as Martin Lee writes in his book “Smoke Signals: A Social History of Marijuana,” “Mikuriya realized that as far as cannabis was concerned he had more in common with the reefer rebels he visited in Northern California than with the ‘repressed bureaucrats’ who debriefed him when he returned from the West Coast.”
In 1968, Mikuriya stepped down from his NIMH position and moved to Berkeley, where he took up a private psychiatric practice. The most important work of his life was about to begin.
As this movement began to take off in California amid the AIDS crisis of the 1980s, Mikuriya came to be seen as the intellectual prowess behind the activist efforts.
San Francisco’s cannabis crusader Dennis Peron was viewed as the key architect of Proposition 215, the 1996 ballot measure that made medical marijuana legal in California, but it was Mikuriya who helped draft the text. If Peron was the father of the medical marijuana movement, Mikuriya was its grandfather, providing guidance behind the scenes.
After the passage of 215, he founded Mikuriya Medical Practice, which lives on today and touts itself as “California’s original medical marijuana consultation service.” During this period, he was writing numerous medical marijuana recommendations for patients every day. He was fondly known to his following as “Dr. Tod.”
In the following years, he would found the California Cannabis Research Medical Group and its latter offshoot, the Society of Cannabis Clinicians.
But his open stance also attracted unwelcome if inevitable attention from the authorities. President Bill Clinton’s hardline drug czar, Gen. Barry McCaffrey, publicly derided Mikuriya’s medical practice and advocacy as “the Cheech and Chong show.”
Finally, in 2000, the Medical Board of California accused Mikuriya of unprofessional conduct for allegedly failing to conduct proper physical examinations on 16 patients for whom he had recommended cannabis. The case was based on the testimony of undercover agents, including police. He would tell the medical board at his disciplinary hearing, “Never before had a fake witness infiltrated my practice and created a fraudulent medical record. It’s most upsetting.”
None of his legitimate patients complained about his conduct — on the contrary, several testified to the Medical Board in his defense.
In 2004, the Medical Board gave Mikuriya five years’ probation and a $75,000 fine. He appealed the ruling, and was allowed to continue practicing under the supervision of the state-appointed monitor.
‘First-line Medication’
Mikuriya died of cancer in May 2007. His obituary in the New York Times noted that he was reported to have recommended cannabis
for nearly 9,000 patients.
And he was quite out of the closet about his own use. As the Los Angeles Times reported in 2004, “He willingly acknowledges, unlike most of his peers in cannabis consulting, that he does indeed smoke pot, mostly in the morning with his coffee.”
As Mikuriya told Ruby Dunes in the interview the year before he died, “Cannabis is far less dangers than most any other medication you can think of, especially when dealing with chronic conditions. Cannabis should be looked on as a first-line medication, instead of it being something that you try when you give up on all the conventional treatments.”
TELL
US, do
you consider cannabis a first-line medication?
The average cannabis user living in states where marijuana is legal has the luxury of stepping inside his or her friendly neighborhood dispensary for access to a variety of pot products, like edible candies, pills, topicals, concentrates and even beverages. These processed variations of the cannabis plant are designed for those consumers who don’t necessarily want to smoke to achieve the desired effect. But when it comes to which method of consumption is best for patients suffering from chronic pain, a new study suggests that loading a bowl full of flower is still the most effective path to getting back to good.
Researchers at the University of New Mexico determined that people trying to manage pain through the use of cannabis are simply better off smoking bud than relying on other forms of the herb. The findings, which were published in the journal Complementary Therapies in Medicine, indicate that “whole cannabis flower was associated with greater pain relief than were other types of products.” The researchers go on to say that “higher tetrahydrocannabinol (THC) levels were the strongest predictors of analgesia and side effects prevalence across the five pain categories.”
These results are especially interesting considering that cannabidiol (CBD), the non-intoxicating compound of the cannabis plant, is now being praised as a rockstar at taming pain. Even the folks pushing the hemp-derived version of this medicine, which is much weaker than the oils made from marijuana, swear that this sometimes truck stop novelty is the key to living pain-free. However, researchers beg to differ. They have concluded that the presence of THC, which produces the stoned effects we all know and love, is also essential if the user expects any discernible pain-relief results.
“Cannabis flower with moderate to high levels of (THC) is an effective mid-level analgesic,” the study reads.
But it just isn’t the existence of THC that makes smoking marijuana the best approach to pain management.
We have swelled into a society convinced that dissecting cannabis and separating its components into good and evil is the right approach to the plant. This is perhaps the reason that CBD has risen to such stardom in the past five years. The problem with this attitude is that it completely disregards the 100 or so other cannabinoids that the cannabis plant has to offer. It also discounts essential terpenes and flavonoids and thereby eliminates any possibility that the patient will benefit from the plant’s synergistic properties. Science established long ago that the entourage effect associated with whole-plant cannabis is what truly provides the therapeutic effects. So, all of you military service members prohibited from using CBD products, don’t worry, you’re definitely not missing much.
But what about kids suffering from epilepsy? Dr. Sanjay Gupta told us years ago that they needed the CBD compound to stop seizures. Sure, while some sick children might have had some luck controlling this affliction through the use of CBD alone, a study published found the compound was more effective at helping them stay seizure-free if it was complemented with just a hint of THC. Researchers found that the closer they got to allowing the two cannabinoids to work together, the better the results. “We saw a statistically significant reduction in motor seizures, and an increase in seizure-free days,” the study authors said.
Although the U.S. Food and Drug Administration (FDA) approved a CBD-based drug called Epidiolex to be prescribed to young patients suffering from two rare forms of epilepsy, not even it is expected to be a miracle cure. The drug, which contains absolutely no THC, is only effective in around 32% of patients, according to the FDA. Parents with epileptic kids have long complained that CBD alone just doesn’t do the trick and that the efficacy of this compound has been hyped beyond belief.
The study out of New Mexico, however, provides some guidance for an America looking for answers as to whether marijuana can relieve pain or not.
A separate study published from the American Society of Anesthesiologists (ASA) shows that 75% of the U.S. population, most of them millennials, has a genuine interest in learning more about how pot can combat pain conditions. These folks, presumably those fed up with all of the anecdotal reports and the conflicting studies that emerge every other week, want to see the federal government finally roll up their sleeves on the cannabis issue and deliver real results.
Unfortunately, it seems that medical marijuana users are going to have to get high before they experience any noticeable pain relief. And that complicates things for a vast majority of the U.S. population — especially those in the workforce. Unlike over-the-counter pain remedies like acetaminophen and ibuprofen, which eliminate some of the hurt without a buzz, smoking marijuana to combat minor aches could lead to impairment issues on the job. Just like most companies don’t allow workers to drink booze on the clock, medical marijuana is not likely to be any different, even after federal legalization finally takes hold. So, don’t sell your stock in Tylenol just yet.
After years of delays, researchers are set to move forward on a landmark clinical trial meant to evaluate the efficacy of smoked medical marijuana in treating post-traumatic stress disorder (PTSD) in military veterans. The study is being funded with tax revenue from legal cannabis sales in Michigan.
The Multidisciplinary Association for Psychedelic Studies, or MAPS, announced this week that the U.S. Food and Drug Administration (FDA) gave approval for Phase 2 of the research, which MAPS described in a press release as “a randomized, placebo-controlled study of 320 Veterans suffering from moderate to severe PTSD who have previously used cannabis.”
The group said the study “is designed to investigate the inhalation of high THC dried cannabis flower, versus placebo cannabis, with the daily dose being self-titrated by participants.” It's meant to reflect consumption patterns already happening across the country and study “the 'real-world' use of inhaled cannabis to understand its potential benefits and risks in treating PTSD.”
MAPS said the project is years in the making, noting that it faced several challenges in clearing the research with the FDA that were only recently resolved.
“After three years of negotiations with the FDA, this decision opens the door to future research into cannabis as a medical treatment, offering hope to millions,” the organization said.
“These data are critical to inform patients, medical providers, and adult-use consumers when considering cannabis in treatment plans for the management of PTSD, pain, and other serious health conditions,” the group's press release said, “yet regulatory obstacles have historically made it difficult or impossible to conduct meaningful research on the safety and effectiveness of cannabis products typically consumed in regulated markets.”
MAPS said that over the years, it responded to five partial clinical hold letters from the FDA that halted the study's progress.
“On August 23, 2024, MAPS responded to the FDA's fifth clinical hold letter by submitting a Formal Dispute Resolution Request (FDRR) to resolve the continued scientific and regulatory disagreement with the Division on four key issues,” according to the organization: “1) the proposed THC dose of the cannabis flower product, 2) smoking as a delivery method, 3) vaping as a delivery method, and 4) the enrollment of cannabis naïve participants.”
After more than three years of tireless effort and five rounds of pushback from FDA, MAPS has won a Formal Dispute Resolution Request (FDRR) with the FDA’s Division of Psychiatry — the same Division that rejected Lykos’ New Drug Application for MDMA-assisted therapy for PTSD.… pic.twitter.com/sUiTjAIV9F
Sue Sisley, a psychiatrist and the principal investigator for the study, said the trial will help shed more light on the scientific legitimacy of using smoked marijuana to treat PTSD. Despite the growing use of cannabis among patients with PTSD and the condition's inclusion in many state medical marijuana programs, she said there's a lack of rigorous data evaluating the treatment's efficacy.
“Within the United States, millions of Americans are smoking or vaporizing cannabis to manage or treat their symptoms,” Sisley said in a statement. “In the absence of high-quality data related to cannabis, much of the information available to patients and regulators is rooted in prohibition and focused only on potential risks, without consideration of potential benefits.”
“In my own practice, Veteran patients have shared how smoking cannabis helped them manage their PTSD symptoms more than traditional pharmaceuticals,” she continued. “Suicide among Veterans is an urgent public health crisis, but it's solvable if we invest in researching new treatments for life-threatening health conditions like PTSD.”
Phase 2 of the research, Sisley said, “will generate data that doctors, like myself, can use to develop treatment plans to help people manage their PTSD symptoms.”
Allison Coker, director of cannabis research at MAPS, said the resolution with the FDA came when the agency said it would allow Phase 2 to proceed with smoked cannabis at commercially available THC levels. Vaporization remains on hold, however, until the FDA can assess the safety of any particular delivery device.
In response to the FDA's separate concern around enrolling cannabis-naive participants in the study, MAPS updated the protocol to require that participants must have “prior experience inhaling (smoking or vaporizing) cannabis.”
FDA had also taken issue with the study's design of allowing self-titration — meaning participants can consume as much cannabis as they choose, up to a certain amount — but MAPS refused to relent on that point.
An FDA spokesperson told the New York Times, which first reported the Phase 2 approval, that she was unable to provide details about what led to the decision but said that the agency “recognizes that there is great need for additional treatment options for mental health conditions such as PTSD.”
The study is being funded by Michigan's Veteran Marijuana Research Grant Program, which uses state revenue from legal cannabis taxes to fund FDA-approved, nonprofit-sponsored clinical trials “researching the efficacy of marijuana in treating the medical conditions of United States armed services veterans and preventing veteran suicide.”
State officials announced $13 million in funding for the research back in 2021, part of a total $20 million grant funding round. Another $7 million that year went to Wayne State University's Bureau of Community Action and Economic Opportunity, which partnered with researchers to study how cannabis might treat a variety of mental health disorders, including PTSD, anxiety, sleep disorders, depression, and suicidality.
In 2022, meanwhile, the Michigan Cannabis Regulatory Agency recommended that year's $20 million go toward two universities: the University of Michigan, where researchers proposed looking at the use of CBD in pain management, and Wayne State University, which was awarded grants for two separate studies: one that billed itself as the “first randomized, controlled, large-scale clinical trial” to examine whether the use of cannabinoids could improve outcomes for veterans with PTSD who are undergoing prolonged exposure (PE) therapy and another into the effects of marijuana on “neuroinflammation and neurobiological underpinnings of suicide ideation in veterans with PTSD.”
The founder and president of MAPS, Rick Doblin, said in the group's announcement of the newly FDA-approved trial that veterans “are in dire need of treatments that can ease their challenging symptoms of PTSD.”
“MAPS takes pride in leading the way to open new research pathways by challenging the FDA to think differently,” he said. “Our cannabis work challenges FDA's typical approach to scheduled dosing and administration of drugs. MAPS refused to compromise the study design in order to fit into the standard box of FDA thinking in order to ensure that cannabis research reflects cannabis use.”
MAPS's past research has included not just cannabis but also, as the group's name suggests, psychedelics. It created a spinoff drug development company, Lykos Therapeutics (formerly MAPS Public Benefit Corporation), that sought FDA approval earlier this year of MDMA to treat PTSD.
“We all feel some type of way about the decision that came out some time ago, and that's OK,” said Leith J. States, chief medical officer at the Office of the Assistant Secretary for Health. “It's indicative of a fact that we're moving forward…and we're doing things in a way that marches us forward in an incremental way.”
While DEA “devised a reasonably inclusive stakeholder assortment” of witnesses, VAC said it still “failed” to fulfill its mandate to allow testimony from interested parties. And the veterans organization said that's evidenced by the fact that Mulrooney has since delayed the formal hearing proceedings until early 2025 because DEA provided insufficient information about their selected witnesses' position on rescheduling or why they should be considered interested parties.
Veterans have taken a lead role in both medical marijuana legalization and the psychedelics reform movement currently unfolding at the state and federal levels. Earlier this year, for example, veterans service organizations (VSOs) pressed members of Congress to urgently pursue the potential benefits of psychedelic-assisted therapy and medical marijuana.
Correction: As the result of an editing error, an earlier version of this story attributed quotes to incorrect members of the MAPS team. Those attributions have been corrected.
Written by Ben Adlinfor Marijuana Moment | Featured image by Anthony Brown/Weedmaps
Over the past four decades, treating diseases with medical marijuana has been on the rise. The credibility of cannabis has grown in the medical community as a possible solution to treat chronic conditions and diseases. While marijuana hasn’t demonstrated that it is the ultimate solution or cure to end a disease in general, it can help soothe the effects of chronic diseases, inhibit diseases from developing at a rapid pace and possibly become a replacement for opioids to handle emotional and physical pain.
This is how marijuana positively contributes to the following seven diseases:
1. Depression
A study from the University of Buffalo’s Research Institute on Addictions tested how marijuana affected chronic stress in rats and used this information to coincide with equivalent human responses. In this experiment, researchers found that when the rats were bound by rodent restraints for long periods of time — a source of chronic stress — the production of their brain’s endocannabinoids rapidly decreased. In regards to human beings in long-term stressful situations, these receptors influence how well a person can process thoughts, gauge emotions and behave, and they even can impact a person’s cognitive ability to handle pain and anxiety. When there is a lack of endocannabinoid production in the brain, an individual is at risk of developing depression. Marijuana can play a role in restoring cannabinoids such as tetrahydrocannabinol and cannabidiol in the endocannabinoid system, and helping ease the depressing.
2. Anxiety
Like depression, anxiety reduces the endocannabinoid production in the brain and inhibits an individual’s ability to cope with pain and stress. However, the use of marijuana to treat anxiety can go either way: It can either deplete anxiety or increase it. While marijuana is meant to bring a person into a tranquil state, some individuals possess a brain chemistry that simply does not react well with the plant’s chemicals. In other cases, marijuana has been able to prevent unwanted anxiety attacks, stimulate a calmer “fight-or-flight response” to stress and all-together provide the user with a “high” that releases any tension in the body.
3. Epilepsy
Given that epilepsy is a cause of seizures (also known as “electrical storms”), medical scientists have created a specific CBD formula that is proven safe for individuals to use because it possessed little to no effect on the sensitive psychoactivity of epilepsy patients. Some of the first tests with marijuana, such as a 2015 test at theNYU Langone Medical Center, actually demonstrated that it had the ability to suppress seizures. Because of this, researchers and developers have been able to manipulate marijuana compounds to tailor to an individual’s epileptic condition, keeping in mind that this disease affects multiple people differently.
4. Alzheimer’s
Marijuana diminishes the intensity of hallucinations, improves poor sleeping habits and stops aggressive outbursts suffered by individuals with Alzheimer’s. The main source of Alzheimer’s is its rapid production of beta-amyloid proteins, which cause plaques to develop in the brain and dangerously reduce the necessary peptides in amino acids that enable one to properly function. Most importantly, marijuana can slow this build-up of proteins to prevent existing Alzheimer’s from deteriorating an individual’s brain.
5. HIV/AIDS
The HIV virus weakens the immune system, but marijuana softens the impact of disorienting and uncomfortable symptoms of a weak immune system, such as nausea, muscle and joint pain, loss of appetite, severe headaches and fevers. Furthermore, in this particular study from Spain in 2008, marijuana was proven to prevent chemical reactions in the body that create HIV compounds.
6. Cancer
While marijuana does not fundamentally cure cancer or diminish its symptoms, it is able to reduce the discomfort in certain treatments that many cancer patients undergo. Cancer patients who use medical marijuana endure a lessened amount of inevitable nausea and vomiting caused by their chemotherapy treatments. Furthermore, cannabinoids improve appetite and can ease the neuropathic pain that is a result of severe nerve damage caused by chemotherapy.
7. Drug Addiction
Though it seems counter-intuitive, recovering addicts can use medical marijuana to reverse the effects of opioid addiction, decrease unwanted drug cravings and even diminish the emotional and physical symptoms of addiction. This is due to the chemical compounds of cannabidiol, which binds to brain receptors that induce a safer “high” and counteract impairments and mental damage caused by long-term drug abuse. Lastly, marijuana can even replace addictive painkillers since it targets the same nerve receptors as opioids without putting the user at risk for chronic addiction.
TELL US, what diseases do you treat with cannabis?
Americans for Safe Access (ASA) has been working for the medical cannabis community and has been a huge voice in the cannabis movement overall for 20 years, which is something we should all be so grateful for. ASA focuses specifically on access to medical cannabis for therapeutic and research purposes, and on the whole medical […]